Choosing Between Fully Ablative and Fractional Laser Resurfacing
Many skin concerns respond well to laser resurfacing, but not every laser is designed to do the same job. The right approach depends on what we are treating, how quickly you need to recover, your skin type, your risk profile, and how much change you want from a single session.
At Midland Skin in Birmingham, your assessment and treatment are carried out by a medical specialist experienced in laser treatment. We work across a full range of technologies in one clinic, including UltraPulse CO₂, UltraClear 2910 nm, Sciton Erbium:YAG 2940 nm, Halo hybrid fractional, and complementary platforms for redness and pigment. That breadth lets us tailor the resurfacing plan around you.Clinical studies show both fully ablative and fractional lasers improve photoageing and scarring through controlled dermal remodelling (Manstein et al, 2004; Hantash et al, 2007).
First principles: how these treatments differ
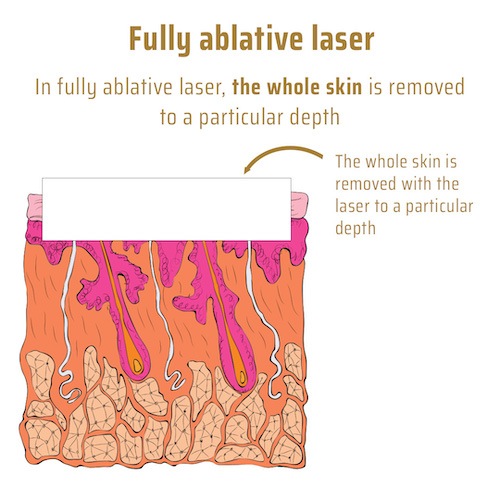
CO₂ or Erbium fully ablative resurfacing
Removes the entire surface layer of skin in the chosen area and a measured portion of the dermis to trigger full regeneration. Best suited to etched lines, advanced photoageing, and deep textural change where comprehensive collagen renewal is required. Typical recovery to new surface skin is about 10–12 days, followed by redness that can last up to 3-6 months. Safest for lighter skin types (Fitzpatrick I and II). Usually a single treatment is required and the effects can last for several years, although some stubborn areas may need a second session. Limiting factors include the possibility of demarcation lines and post-inflammatory hyperpigmentation.
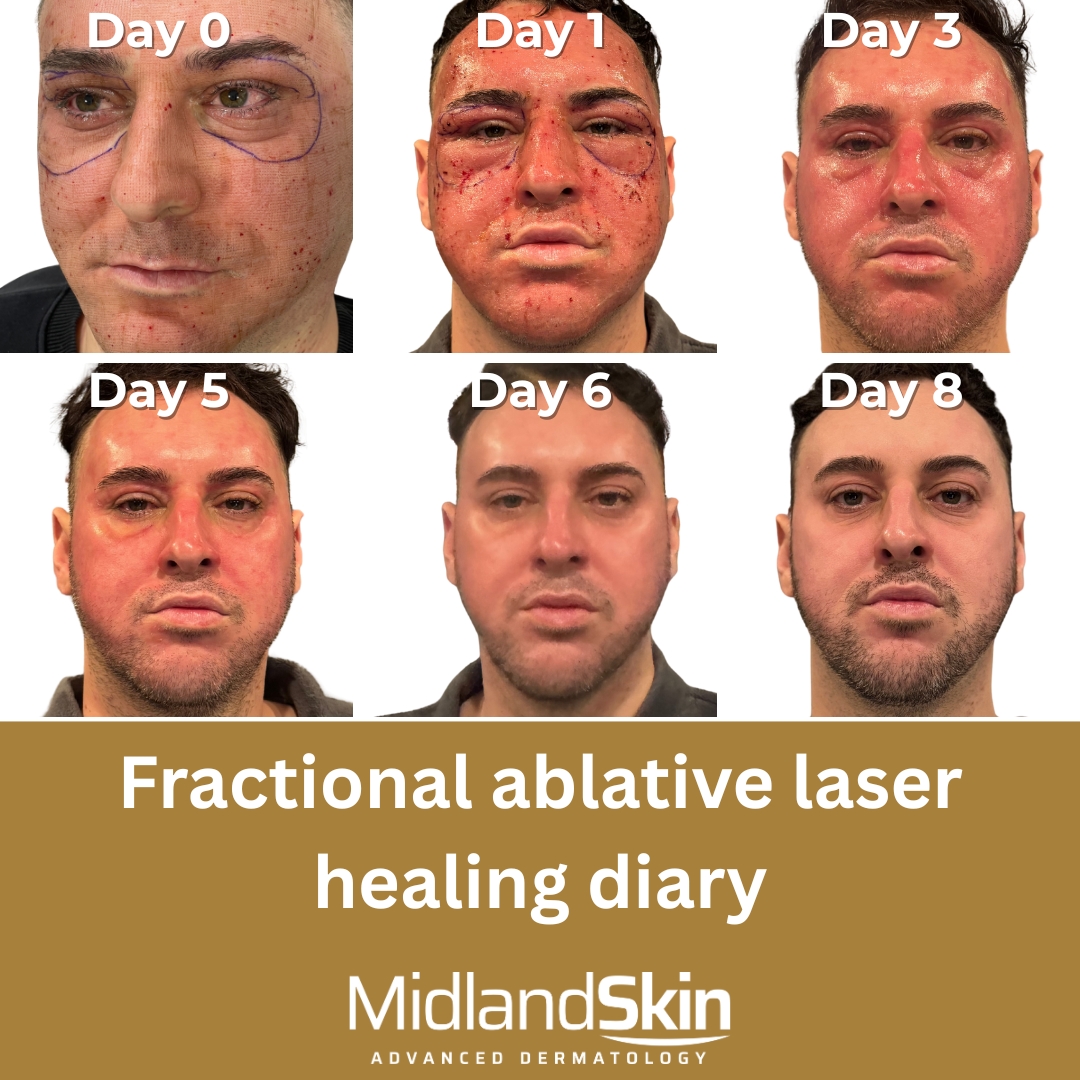
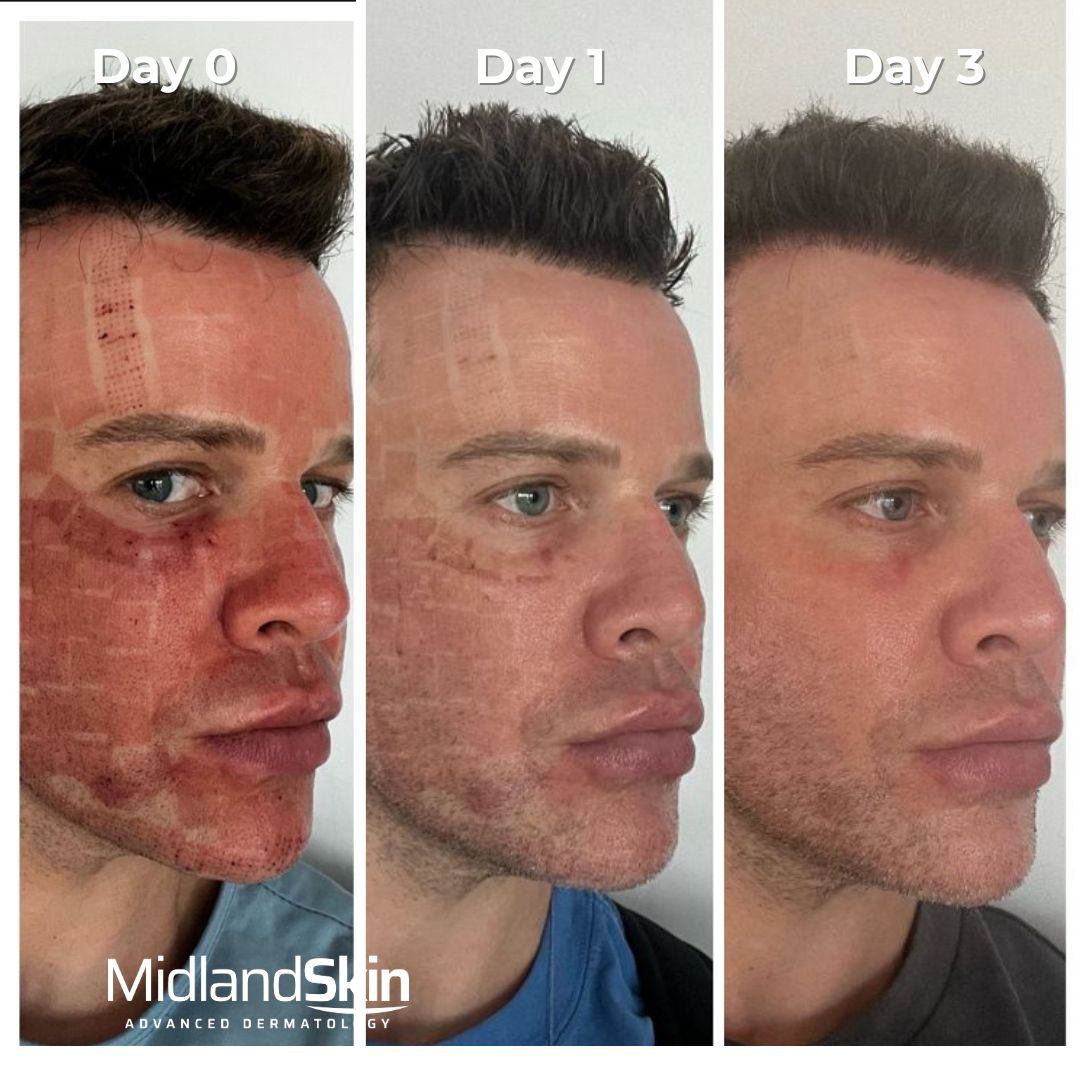
Fractional ablative resurfacing (CO₂, Erbium:YAG and 2910 nm)
Treats a pattern of microscopic columns while leaving bridges of untouched skin to speed healing. Depth and density can be adjusted for acne scarring, lines, pores and texture. Recovery usually takes 5–9 days and is shorter than fully ablative resurfacing. Because only a fraction of the skin is treated, side effects are fewer than with fully ablative resurfacing. Treatment is typically repeated for optimal results. For rejuvenation, plan 2 sessions about 8 weeks apart. For acne scarring, plan sessions about 12 weeks apart.
Fractional CO₂ and Er:YAG lasers deliver columns of thermal injury that stimulate collagen production while leaving surrounding skin intact, allowing faster recovery (Manstein et al, 2004). The degree of improvement and downtime depend on the energy, density, and number of passes used.
Fractional non-ablative resurfacing (for example Halo 1470 nm)
Heats the dermis to stimulate collagen without removing the surface. Useful for early photoageing, fine textural change and maintenance when downtime must be minimal. Usually planned as a course of 2 treatments for rejuvenation.
CO₂ or Erbium for ablative work?
CO₂ tends to give stronger tightening and wrinkle softening because of greater thermal effect.
Erbium (2940 nm and 2910 nm) ablates very efficiently with less residual heat, which can mean a quicker return to normal barrier function and potentially lower pigment risk when used appropriately. Heat can be increased to emulate CO₂ where suitable.
What results can you expect?
Severe etched lines, wrinkles, eyelid laxity, solar elastosis: Fully ablative resurfacing remains the most powerful single procedure in lighter skin types. Fractional ablative approaches also achieve meaningful softening with less recovery time when fully ablative is not appropriate or desired.
Acne scars (rolling, boxcar and mixed): Fractional CO₂ and fractional Erbium both improve atrophic scars. We often combine with subcision, TCA CROSS and, where appropriate, volume restoration.
Pores, texture and dullness: Fractional Erbium or hybrid fractional options refine texture with steady gains in brightness, plumpness and evenness.
Pigment and redness as part of photoageing: Often managed with staged care, usingFractional CO₂ or fractional Erbium resurfacing alongside targeted pigment or vascular treatments such as BBL.
Skin cancer prevention: Any form of resurfacing fully ablative or fractional will do this
Downtime at a glance
Treatment style
Typical sessions
Time to new surface skin
Social downtime guidance
Fully ablative CO₂ or Erbium laser resurfacing
1
~7-10 days
14-21 days
Fractional ablative (CO₂ or Erbium)
2–3
4–7 days
5–10 days
Fractional non-ablative
3–5
0–4 days
~5–7 days
Everyone heals at their own pace. Allow enough time to heal without pressure.
Fully ablative laser resurfacing healing diary
This patient took about 9 days for the skin to reform, and about 2 weeks before she was able to work from home or start going out.
Safe laser resurfacing in darker skin types is possible with the right device, parameters and aftercare. Fractional Erbium and low-density fractional CO₂ may be used in darker skin types (Fitzpatrick III–V) with conservative energy and longer recovery intervals. CO₂ remains highly effective too in darker skin types, and selection and aftercare are critical.
Safety, preparation and aftercare
Consultant-led planning: Treatment depth is matched to the goal and to delicate anatomy around the eyes and lips.
Cold-sore prevention: Antivirals are used where there is a history of herpes simplex.
Pigment-risk preparation: Careful aftercare to reduce post-inflammatory hyperpigmentation.
Healing support: Regular cleansing, bland occlusive emollients, and strict sun avoidance. Prescription products are introduced if clinically indicated.
Possible side effects: Temporary redness, swelling, crusting or bronzing, milia, acne flares and pigment change. Infection and scarring are uncommon with good selection and aftercare but remain important risks we discuss in full.
Comparing fully ablative and fractional resurfacing
Fully ablative laser resurfacing
Fractional laser resurfacing
Suitable skin types
I–II
I–V
Redness duration
3–6 months
2–6 weeks
Swelling
3–6 days
1–3 days
Pain after procedure
1–2 days
0–1 day
Weeping
~3 days
~1–2 days
Lines of demarcation
Possible
Less likely
Grid marks
Unlikely
Occasional
Post-inflammatory hyperpigmentation
Possible
Possible
Sun protection essential
6-12 months
3-6 months
Skin sensitivity
4–6 weeks
3–6 months
How we choose which laser
Fully ablative treatment is usually chosen when deep structural change is required and downtime can be accommodated. Fractional resurfacing suits moderate texture change or when downtime must be shorter. The choice depends on the patient’s goals, lifestyle, skin type, and tolerance for risk.
Map the problem: Are the concerns etched lines, mixed acne scarring, or general photoageing?
Match the tool: Pick CO₂, Erbium or hybrid fractional based on area, depth and skin type.
Set parameters: Adjust coverage and depth to balance risk profile, skin type and downtime.
Plan the journey: One definitive session or a staged approach, with clear aftercare and check-ins.
Combination treatment: Combination protocols (e.g. fractional + fully ablative spot treatment) can balance impact with healing, and are supported by histological studies of depth-controlled ablation
Some examples
62-year-old female, skin type II, with etched upper-lip lines, solar elastosis and eyelid ageing: fully ablative resurfacing (CO₂ or Erbium, or combined).
29-year-old male, skin type III, seeking maintenance and brightness: Halo or UltraClear.
33-year-old female, skin type I, early eyelid ageing: two sessions of fractional CO₂ around the eyes, with light resurfacing to the face.
24-year-old male, skin type V, with acne scarring: fractional CO₂, Erbium:YAG, UltraClear or Halo.
49-year-old female, skin type IV, seeking rejuvenation with limited downtime: UltraClear or Halo/BBL.
Frequently asked questions
Will this help movement-related lines?
Lasers improve surface lines and texture. Dynamic lines caused by muscle movement usually respond better to targeted injectables. Combination plans are common.
How quickly will I see results?
Freshening is seen within weeks of healing. The full collagen response can take 3–6 months.
Can you guarantee results?
No medical treatment can guarantee a particular outcome. It is important to have realistic expectations. A small number of people may not respond as well as hoped.
How long will the improvement last?
Structural gains from ablative resurfacing are long-lasting. Skin will continue to age, so good skincare, sun protection and occasional maintenance help preserve results.
Can I combine treatments?
Yes. For acne scarring we often combine subcision, fractional laser and TCA CROSS. For photoageing we may add targeted vascular or pigment treatment.
Why Midland Skin
Consultant dermatologists only: You see the most qualified clinician for assessment and treatment.
All major technologies in one place: UltraPulse CO₂, UltraClear 2910 nm, Sciton Er:YAG, Halo and more, so we are not locked to a single device.
Care for every skin type: Parameter sets and aftercare adapted for skin of colour and sensitive skin.
Clear, realistic planning: A written plan explains what to expect at each stage.
Next steps
Book a consultation to discuss your skin, goals and timetable. We will examine your skin, explain what each option can and cannot do, and agree a plan that fits your life.
Manstein D, Herron GS, Sink RK, Tanner H, Anderson RR. Fractional photothermolysis: a new concept for cutaneous remodelling. Lasers Surg Med. 2004;34(5):426-438.
Hantash BM, Bedi VP, Kapadia B, et al. Ex vivo histological evaluation of a novel ablative fractional resurfacing device. Lasers Surg Med. 2007;39(2):87-95.
Sadick NS, Weiss RA. Laser resurfacing: classifying the different technologies. J Cosmet Dermatol. 2001;1(1):36-42.
Alster TS, Lupton JR. Lasers in dermatology: The role of ablative and non-ablative resurfacing. Curr Treat Options Dermatol. 1996;2(1):39-48.
Moradi A, Navarrete-Dechent C, Nguyen T, et al. Safety of ablative fractional laser resurfacing in darker skin phototypes: A systematic review. Dermatol Surg. 2021;47(6):820-827.
Disclaimer
This article provides general information only and is not a substitute for personalised medical advice.
Author: Dr Sajjad Rajpar, Consultant Dermatologist (GMC Specialist Register) Publish date: 6 October 2025 Last reviewed: 6 October 2025
About the Author
This page has been written and/or medically reviewed by Dr Sajjad Rajpar, Consultant Dermatologist and Medical Director of Midland Skin, Birmingham.
Dr Rajpar is on the GMC Specialist Register in Dermatology and has over 20 years’ experience in clinical dermatology. He provides clinical oversight to ensure the information on this page is accurate, balanced and consistent with current dermatology practice.
Dr Sajjad Rajpar
Date last updated: 26th Oct 2025
Book in with us
Pellentesque arcu cras cursus nascetur felis id sem gravida. Tellus lobortis eu erat in pellentesque ultrices. Egestas nunc iaculis massa turpis nulla.