Suspicious Mole? Private vs NHS: What Happens and How Fast
TL;DR: A changing mole needs prompt, expert assessment. On the NHS, you are triaged against national cancer standards, including the Faster Diagnosis Standard. Privately at Midland Skin, you are seen by an experienced consultant dermatologist on the GMC Specialist Register, not by a photographer, nurse or a trainee doctor. Expect dermoscopy, clear advice, and, where appropriate, swift biopsy under local anaesthetic.Most UK histology reports return in about two weeks, although timing varies by provider and laboratory workload. The best route is the one that gets you a high-quality opinion quickly and a clear plan.
The worry behind a changing mole and why speed matters
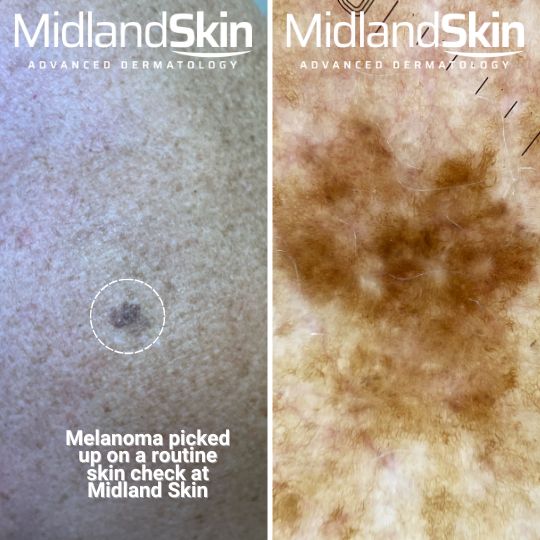
A new or changing mole can trigger understandable what-if thoughts. In clinic, we describe a lesion as suspicious when its pattern, colour, border or evolution suggests risk. The first-line tool is dermoscopy, a magnified and polarised light examination that improves accuracy over unaided visual inspection for identifying melanoma and ruling out false alarms.
Two routes, one goal: catching cancer early
NHS standards in plain English
Urgent referrals in England are managed against the Faster Diagnosis Standard, which aims for a diagnosis or ruling out cancer within a set timeframe, alongside 31-day and 62-day treatment measures. Frequently you are referred to a teledermatology clinic following which you are directed to the right clinic based on risk, examined with dermoscopy, and given a plan that may include a biopsy. Sometimes you are sent directly from a teledermatology clinic to a biopsy procedure.
The private pathway at Midland Skin
Privately, you choose timing that is prompt and suits you and consultant led care. At Midland Skin you are seen by a consultant dermatologist for a consultant-led dermoscopic assessment. If a biopsy is indicated, we discuss the most suitable technique, such as punch, shave or excision, and arrange it promptly under local anaesthetic with clear aftercare and a plan for results. The biopsy is often done on the same day as your consultation.
At-a-glance timelines: NHS vs private for a suspicious mole
NHS (typical flow): GP urgent referral → teledermatology → hospital dermatology clinic → dermoscopy and decision → biopsy on the day or booked → histology result → management plan.
Private at Midland Skin (typical flow): self-referral → consultant-led dermoscopy → biopsy or excision under local anaesthetic (arranged promptly when appropriate) → histology result → management plan. Most labs report within about 1–2 weeks, but timing varies by provider and laboratory workload.
Your first assessment: what actually happens
We begin with your story: what changed, when you noticed it, any symptoms such as itch or bleeding, personal or family skin cancer history, and sun exposure. Then we examine the lesion and, when relevant, the surrounding skin. Dermoscopy reveals subsurface colours and structures that guide whether to watch, image or biopsy. Dermoscopy outperforms visual inspection alone.
If you prefer a focused expert check with dermoscopy, you can book a consultant-led appointment here: Mole checks at Midland Skin.
Other moles can also be checked at your initial private consultation and you can even opt to have a full head to toe skin check.
Teledermatology vs face-to-face
Good photographs, sometimes with dermoscopic images, can help triage and prioritise. Accuracy depends on image quality and clinical context. When there is uncertainty, an in-person dermoscopic assessment remains the safer choice.
Biopsy choices, scarring and safety: practical questions
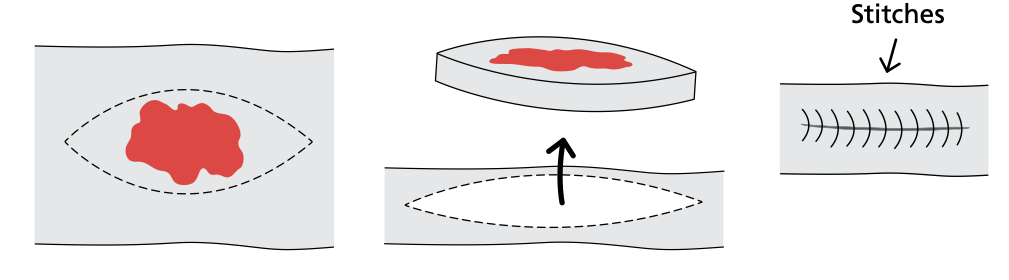
Excision removes the whole lesion with a margin. This is preferred when melanoma is suspected.
Punch biopsy takes a core sample and is useful in specific diagnostic scenarios.
Shave biopsy removes a superficial sample and is used selectively when appropriate.
All are done under local anaesthetic with clear wound-care advice. Any cut leaves a scar, yet careful planning of technique and closure helps minimise impact.
For a plain-English overview of what minor procedures involve under local anaesthetic, see: Minor skin surgery.If the mole appears benign but causes problems such as snagging, catching or bleeding, we can discuss removal for comfort or function: Mole removal options
Suspicious moles are removed whole and the wound is stitched together to leave a stitched scar.
Is Mohs for moles? Clearing up a common misconception
Mohs micrographic surgery removes tissue in stages with same-day microscopic margin checks. It maximises cure while sparing normal skin. In the UK it is used mainly for selected basal cell carcinomas (BCCs) and some squamous cell carcinomas in high-risk sites. It is not the standard approach for a suspicious pigmented lesion where melanoma is a concern.
For more on BCC itself, including symptoms, risks and treatment pathways, see: Basal cell carcinoma (BCC).
If you have been advised Mohs for a confirmed BCC, this page explains how it works in practice: Mohs micrographic surgery.
Results and next steps: how long and what they mean
Most private UK histopathology reports for routine cancer-pathway biopsies return in about two weeks. Timing varies with provider processes, laboratory workload and any extra tests that may be needed. Your report guides the next step: reassurance and discharge if benign, or wider excision, mapping or surveillance if malignant or atypical.
Choosing NHS or private: a simple decision aid
Risk and urgency: if melanoma is a concern, prioritise a prompt, high-quality dermoscopic assessment and a clear next step.
Control and timing: if choosing a specific consultant dermatologist and a predictable appointment lowers anxiety and speeds decisions, private care may suit you.
Complexity: previous melanoma, high-risk sites or multiple changing lesions often benefit from consultant-led review.
Practicalities: consider travel, recovery time and help with aftercare.
Continuity: you can move between routes; what matters is fast, expert assessment and clear communication.
We see patients in Birmingham, Solihull, Sutton Coldfield and Edgbaston and support people across the West Midlands, with online advice across the UK where appropriate.
FAQs
Will the NHS remove a benign mole?
Generally, cosmetic benign lesions are not removed on the NHS. Suspicious lesions are assessed and biopsied if needed on a cancer pathway.
How long do mole biopsy results take in the UK?
Often around two weeks for straightforward cases. It depends on laboratory workload and whether extra tests are required. We set expectations clearly for your case.
Can I switch between NHS and private?
Yes. You can have an assessment privately and still choose NHS or private treatment, providing the concern you seek treatment for is routinely provided in the NHS.
Is teledermatology as good as face-to-face for moles?
Teledermatology is helpful for triage, yet image quality and context may limit accuracy. When there is uncertainty, in-person dermoscopy is safer.
Is Mohs surgery used for suspicious moles?
No. Mohs is mainly for selected BCCs and some SCCs. It is not standard for suspected melanoma.
Key takeaways
A changing mole needs prompt, expert assessment with dermoscopy.
Consultant-led review at Midland Skin means you see a GMC-registered consultant dermatologist, not a nurse or trainee.
If a biopsy is needed, we choose the technique that answers the clinical question and minimises scarring.
Most histology reports return in about one to two weeks, although timing varies. Expectations are set clearly.
Mohs is for selected BCCs, not suspicious pigmented lesions.
Disclaimer
This article provides general information only and is not a substitute for personalised medical advice. If you notice a fast-changing, bleeding or very dark lesion, arrange an urgent medical assessment.
Author: Dr Sajjad Rajpar, Consultant Dermatologist (GMC Specialist Register) Publish date: 6 October 2025 Last reviewed: 6 October 2025
References
Chuchu, N., Dinnes, J., Takwoingi, Y., Matin, R., Bayliss, S. E., Davenport, C., & Deeks, J. J. (2018). Teledermatology for diagnosing skin cancer in adults. Cochrane Database of Systematic Reviews, 2018(12), CD013193. https://doi.org/10.1002/14651858.CD013193
Dinnes, J., Deeks, J. J., Chuchu, N., Saleh, D., Bayliss, S. E., Patel, L., Davenport, C., & Matin, R. (2018). Dermoscopy, with and without visual inspection, for diagnosing melanoma in adults. Cochrane Database of Systematic Reviews, 2018(12), CD011902. https://doi.org/10.1002/14651858.CD011902.pub2
Nasr, I., Bichakjian, C. K., Dika, E., et al. (2021). British Association of Dermatologists guidelines for the management of adults with basal cell carcinoma. British Journal of Dermatology, 185(5), 899–920. https://doi.org/10.1111/bjd.20524
About the Author
This page has been written and/or medically reviewed by Dr Sajjad Rajpar, Consultant Dermatologist and Medical Director of Midland Skin, Birmingham.
Dr Rajpar is on the GMC Specialist Register in Dermatology and has over 20 years’ experience in clinical dermatology. He provides clinical oversight to ensure the information on this page is accurate, balanced and consistent with current dermatology practice.
Dr Sajjad Rajpar
Date last updated: 6th Nov 2025
Book in with us
Expert, consultant led care in dermatology, skin surgery, eyelid surgery, lasers and aesthetics.